
Asthma And Vitamin D Deficiency In Adults
Practice Essentials
Vitamin D deficiency can result from inadequate exposure to sunlight; malabsorption; accelerated catabolism from certain medications; and, in infants, the minimal amount of vitamin D found in breast milk. In children, vitamin D deficiency can result in rickets, which presents as bowing of the legs; in adults, it results in osteomalacia, which presents as a poorly mineralized skeletal matrix. See the image below.
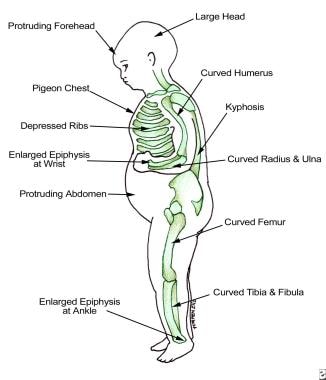
Findings in patients with rickets.
Signs and symptoms
Vitamin D deficiency is often clinically silent. Manifestations are as follows:
-
Children are often found to have started walking late or prefer to sit down for prolonged periods
-
Adults can experience chronic muscle aches and pains
Physical findings in severe vitamin D deficiency are as follows:
-
In children, bowing in the legs
-
In adults, periosteal bone pain, best detected with firm pressure on the sternum or tibia
See Clinical Presentation for more detail.
Diagnosis
Measurement of serum 25-hydroxyvitamin D (25[OH]D) is the best test to determine vitamin D status. Levels of 25(OH)D are interpreted as follows [1] :
-
21-29 ng/mL (52.5-72.5 nmol/L): Vitamin D insufficiency
-
< 20 ng/mL (< 50 nmol/L): Vitamin D deficiency
Although not always required for the diagnosis of vitamin D insufficiency, measurement of the serum parathyroid hormone (PTH) level may help establish the diagnosis of vitamin D insufficiency. PTH levels are often elevated in patients with vitamin D insufficiency, indicating secondary hyperparathyroidism.
Screening for vitamin D deficiency is recommended only in those individuals who are at high risk for vitamin D deficiency, including the following [2] :
-
Patients with osteoporosis
-
Patients with a malabsorption syndrome
-
Black and Hispanic individuals
-
Obese persons (body mass index >30 kg/m2) [3]
-
Patients with disorders that affect the metabolism of vitamin D and phosphate (eg, chronic kidney disease)
See Workup for more detail.
Management
Recommended treatment for vitamin D–deficient patients up to 1 year of age is as follows [2] :
-
2000 IU/day of vitamin D2 or D3 for 6 weeks or
-
50,000 IU of vitamin D2 or D3 once weekly for 6 weeks
-
When the serum 25(OH)D level exceeds 30 ng/mL, provide maintenance treatment of 400-1000 IU/day
Recommended treatment for vitamin D–deficient patients 1–18 years of age is as follows [2] :
-
2000 IU/day of vitamin D2 or D3 for at least 6 weeks or
-
50,000 IU of vitamin D2 once weekly for at least 6 weeks
-
When the serum 25(OH)D level exceeds 30 ng/mL, provide maintenance treatment of 600-1000 IU/day
Recommended treatment for vitamin D–deficient adults is as follows [2] :
-
50,000 IU of vitamin D2 or D3 once weekly for 8 weeks or
-
6000 IU/day of vitamin D2 or D3 for 8 weeks
-
When the serum 25(OH)D level exceeds 30 ng/mL, provide maintenance treatment of 1500-2000 IU/day
Recommended treatment for vitamin D–deficient patients who are obese, have a malabsorption syndrome, or are taking medication that affects vitamin D metabolism, is as follows [2] :
-
At least 6000-10,000 IU of vitamin D daily
-
When the serum 25(OH)D level exceeds 30 ng/mL, provide maintenance treatment of 3000-6000 IU/day
If the 25(OH)D concentration remains persistently low despite several attempts at correction with oral vitamin D, a trial of ultraviolet B light therapy (ie, by tanning lamps) may be considered to improve vitamin D status.
Prevention
Unprotected sun exposure is the major source of vitamin D for both children and adults. [2] Provision of vitamin D from sunlight is as follows:
-
Sensible sun exposure, especially between the hours of 10 am and 3 pm, produces vitamin D in the skin that may last twice as long in the blood compared with ingested vitamin D [4]
-
Full-body sun exposure producing slight pinkness in light-skinned persons results in vitamin D production equivalent to ingesting 10,000-25,000 IU [5]
-
Increased skin pigmentation, aging, and sunscreen use reduce the skin's vitamin D3 production
Recommended dietary intake of vitamin D for patients at risk of vitamin D deficiency is as follows [2] :
-
In infants and children up to 1 year old, at least 400 IU/day, to maximize bone health
-
In children and adolescents 1-18 years of age, at least 600 IU/day to maximize bone health
-
In adults 19-50 years of age, at least 600 IU/day to maximize bone health and muscle function
-
Raising the serum 25(OH)D level consistently above 30 ng/mL may require vitamin D intake of at least 1000 IU/day
-
Whether recommended levels of vitamin D intake will provide all the potential nonskeletal health benefits associated with vitamin D is currently unknown
Most dietary sources of vitamin D do not contain sufficient amounts of the vitamin to satisfy daily requirements. The following foods contain the indicated amounts of vitamin D, as reported by the US Department of Agriculture's (USDA's) Nutrient Data Laboratory:
-
Fortified milk (8 oz) - 100 IU
-
Fortified orange juice (8 oz) [6] - 100 IU
-
Fortified cereal (1 serving) - 40-80 IU
-
Pickled herring (100 g) - 680 IU
-
Canned salmon with bones (100 g) - 624 IU
-
Mackerel (100 g) - 360 IU
-
Canned sardines (100 g) - 272 IU
-
Codfish (100 g) - 44 IU
-
Swiss cheese (100 g) - 44 IU
-
Raw shiitake mushrooms (100 g) - 76 IU
-
Most multivitamins (1 tab) - 400 IU
See Treatment and Medication for more detail.
![]()
Background
Vitamin D deficiency in children can manifest as rickets (it is the most common cause of nutritional rickets), which presents as bowing of the legs. Vitamin D deficiency in adults results in osteomalacia, which presents as a poorly mineralized skeletal matrix. These adults can experience chronic muscle aches and pains (see the images below). [7] (See Presentation and Prognosis.)
Findings in patients with rickets.

Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
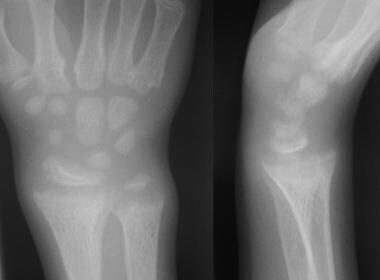
Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
Vitamin D is important for calcium homeostasis and for optimal skeletal health. The major function of vitamin D is to increase the efficiency of calcium absorption from the small intestine. Heaney and colleagues demonstrated that maximum calcium absorption occurs at levels of 25-hydroxyvitamin D (25[OH]D) greater than 32 ng/mL. [8] (See Pathophysiology and Etiology.)
Vitamin D also enhances the absorption of phosphorus from the distal small bowel. Adequate calcium and phosphorus absorption from the intestine is important for proper mineralization of the bone. The second major function of vitamin D is involvement in the maturation of osteoclasts, which resorb calcium from the bones. (See Pathophysiology and Etiology.)
The term vitamin D refers to either vitamin D2 or vitamin D3. Vitamin D3, also known as cholecalciferol, is either made in the skin or obtained in the diet from fatty fish. Vitamin D2, also known as ergocalciferol, is obtained from irradiated fungi, such as yeast. Vitamin D2 and vitamin D3 are used to supplement food products or are contained in multivitamins. (See Treatment and Medication.)
Past studies suggested that vitamin D3 may be more effective than vitamin D2 in establishing normal vitamin D stores. [9, 10] However, a study by Holick and colleagues demonstrated that vitamin D2 and vitamin D3 appear to be equipotent in raising 25(OH)D concentrations when they are given in daily doses of 1000 IU. [11]
Vitamin D deficiency during pregnancy affects offspring. In a community-based study of 901 mother and offspring pairs, researchers found that maternal vitamin D deficiency (serum 25-hydroxyvitamin D < 50 nmol/L) at 18 weeks' pregnancy was associated with impaired lung development at age 6 in offspring, neurocognitive difficulties at age 10, increased risk of eating disorders in adolescence, and lower peak bone mass at age 20. [12, 13, 14]
Findings suggest that vitamin D plays an active role in fetal development, particularly the development of the brain, lungs, and bones.
Physiology
The production of vitamin D3 in the skin involves a series of reactions initiating with 7-dehydrocholesterol. Upon exposure to ultraviolet B (UVB) radiation between the wavelengths of 290-315 nm, 7-dehydrocholesterol is converted to previtamin D3, which is then converted to vitamin D3 after a thermally induced isomerization reaction in the skin. From the skin, newly formed vitamin D3 enters the circulation by binding to vitamin D binding protein (DBP). In order to become active, vitamin D requires 2 sequential hydroxylations to form 1,25-dihydroxyvitamin D (1,25[OH]2 D).
Vitamin D is initially hydroxylated in the 25 position by the hepatic microsomal and/or mitochondrial enzyme vitamin D 25-hydroxylase. The second hydroxylation occurs in the kidney and is performed by the P450 enzyme 25-hydroxyvitamin D-1 alpha-hydroxylase.
Upon entering the cell, the 1,25(OH)2 D hormone binds to the vitamin D receptor (VDR). The bound vitamin D receptor then forms a heterodimer with the retinoic acid X receptor (RXR). This heterodimer then goes to the nucleus to bind deoxyribonucleic acid (DNA) and increases transcription of vitamin D–related genes.
![]()
Pathophysiology
Inadequate circulating 25(OH)D is associated with elevated parathyroid hormone (PTH); this condition is called secondary hyperparathyroidism. The rise in PTH may result in increased mobilization of calcium from the bone, which leads to decreased mineralization of the bone.
Of note, prolonged exposure to the sun does not cause vitamin D toxicity. This is because after prolonged UVB radiation exposure, the vitamin D made in the skin is further degraded to the inactive vitamin D metabolites tachysterol and lumisterol.
As strongly suggested by genetic, molecular, cellular, and animal studies, extraskeletal effects related to vitamin D signaling include roles in cell proliferation, immune and muscle function, skin differentiation, and reproduction, with vitamin D having vascular and metabolic actions as well. Observational studies have pointed to a relationship between poor vitamin D status and almost all diseases connected to these extraskeletal influences. However, while randomized, controlled trials and Mendelian randomization studies have indicated that vitamin D supplementation can lower the incidence of some disorders, only mixed conclusions on the matter have been reached globally. [15]
![]()
Etiology
Vitamin D deficiency can result from the following:
-
Inadequate exposure to sunlight - This causes a deficiency in cutaneously synthesized vitamin D; adults in nursing homes or health care institutions are at a particularly high risk. [16]
-
Vitamin D malabsorption problems - People who have undergone resection of the small intestine are at risk for this condition; diseases associated with vitamin D malabsorption include celiac sprue, short bowel syndrome, [17] and cystic fibrosis. [18]
-
Minimal amounts of vitamin D in human breast milk - The American Academy of Pediatrics recommends vitamin D supplementation starting at age 2 months for infants fed exclusively with breast milk. [19]
-
Medications - Some medications are associated with vitamin D deficiency; drugs such as Dilantin, phenobarbital, and rifampin can induce hepatic p450 enzymes to accelerate the catabolism of vitamin D.
![]()
Epidemiology
Occurrence in the United States
Vitamin D insufficiency is highest among people who are elderly, institutionalized, or hospitalized. In the United States, 60% of nursing home residents [20] and 57% of hospitalized patients [21] were found to be vitamin D deficient.
However, vitamin D insufficiency is not restricted to the elderly and hospitalized population; several studies have found a high prevalence of vitamin D deficiency among healthy, young adults. A study determined that nearly two thirds of healthy, young adults in Boston were vitamin D insufficient at the end of winter. [22]
An analysis of data on 2877 US children and adolescents (age, 6-18 y) from the National Health and Nutrition Examination Survey (NHANES) 2003-2006 indicated that, based on current Institute of Medicine Committee guidelines, about 10.3% of this population (an estimated 5.5 million) had inadequate vitamin D (25(OH)D) levels (< 16 ng/mL), and 4.6% (an estimated 2.5 million) had levels placing them at risk of frank deficiency (< 12 ng/mL). [23, 24] Adolescents (age, 14-18 y) and obese children had the highest risk of 25(OH)D deficiency and inadequacy, and these risks were also higher among girls than boys (of any age and body mass index) and among nonwhite children. [24]
Vitamin D status may fluctuate throughout the year, with the highest serum 25(OH)D level occurring after the summer and the lowest serum 25(OH)D concentrations after winter. A study by Shoben at el demonstrated that mean serum 25(OH)D concentrations can vary as much as 9.5 ng/mL. Factors such as male sex, higher latitude, and greater physical activity levels were found to be associated with greater differences in serum 25(OH)D concentrations in winter and summer. [25]
International occurrence
Similar rates of vitamin D deficiency have been reported in Europe [26] and Canada. A greater prevalence of vitamin D deficiency exists in Middle Eastern countries. A study of 316 young adults aged 30-50 years from the Middle East showed that 72.8% had 25(OH)D values of less than 15 ng/dL (that is, severely deficient). This was significantly more common in women than in men (83.9% vs 48.5%, respectively). The difference between sexes probably reflects the cultural and religious practices leading to less skin exposure in women than in men. [27, 28, 29, 30]
Race-related demographics
Darker skin interferes with the cutaneous synthesis of vitamin D. A study by Holick and coauthors demonstrated that non-Hispanic black subjects require 6 times the amount of UV radiation necessary to produce a serum vitamin D concentration similar to that found in non-Hispanic white subjects. [31] The explanation for the increased radiation necessary to increase vitamin D levels is that melanin absorbs ultraviolet radiation.
The decreased efficacy of vitamin D production by darker-pigmented skin explains the higher prevalence of vitamin D insufficiency among darker-skinned adults. Dawson-Hughes and colleagues demonstrated that in Boston, 73% of elderly black subjects were vitamin D insufficient, compared with 35% of elderly non-Hispanic whites. [32]
In a large survey of 1500 healthy black women younger than 50 years, 40% were vitamin D deficient (25[OH]D < 16ng/mL), compared with 4% of 1400 white women in that study. [33]
Age-related demographics
Vitamin D production in the skin declines with advancing age, making elderly populations more dependent on dietary vitamin D. For the average older person, higher dietary intake of vitamin D may be required to achieve optimal serum levels of 25(OH)D. [34]
![]()
Prognosis
The treatment of vitamin D insufficiency can decrease the risk of hip and nonvertebral fractures. [35, 36] A meta-analysis by Boonen et al of postmenopausal women and of men aged 50 years or older reporting a risk of hip fracture found that oral vitamin D supplementation reduced the risk of hip fractures by 18% when vitamin D and calcium were taken together. [37] Most of the trials that demonstrated the antifracture efficacy of vitamin D used approximately 800 IU of vitamin D3. The minimum 25(OH)D level at which antifracture efficacy was observed was 30 ng/ml (74 nmol/L), suggesting a threshold for optimal levels of 25(OH)D for fracture protection.
Results from another meta-analysis, evaluating the efficacy of oral vitamin D supplementation in the prevention of hip and other nonvertebral bone fractures in individuals aged 65 years or older, indicated that vitamin D offers dose-dependent fracture protection. [38] The analysis, by Bischoff-Ferrari et al, took into account 12 double-blind, randomized, controlled trials (RCTs) for nonvertebral fractures (n = 42,279) and 8 RCTs for hip fractures (n = 40,886), comparing the results obtained from the use of oral vitamin D (with or without calcium) with those derived from the administration of calcium alone and from placebo use.
In this study, doses of more than 400 IU/day were found to reduce fractures by at least 20% in individuals aged 65 years or older. [38] In contrast to the Boonen study, the investigators maintained that these effects were independent of calcium supplementation.
Vitamin D insufficiency contributes to osteoporosis by decreasing intestinal calcium absorption. [8, 39] Treatment of vitamin D deficiency has been shown to improve bone mineral density. [40, 41] An analysis of the Third National Health and Nutrition Examination Survey (NHANES III) demonstrated a positive correlation between circulating 25(OH)D levels and bone mineral density. [42]
Vitamin D supplementation has been associated with a reduction in falls and improved muscle strength in the elderly. A meta-analysis demonstrated that vitamin D supplementation resulted in a reduction in falls of about 22% in ambulatory and institutionalized elderly subjects, as compared with controls. [43, 44] Another meta-analysis examining muscle strength associated with vitamin D supplementation found significant improvement in reduced postural sway, timed up-and-go test results, and lower extremity strength in a pooled analysis of 13 studies. [45]
Epidemiologic data suggest that vitamin D deficiency places adults at risk for developing cancer [46, 47, 48, 49, 50] ; these apparently include breast, colon, and prostate cancer. [51, 52] Several studies using cultured cancer cells in mice models have also supported the notion that vitamin D prevents the growth of cancers. [53] Larger, randomized clinical trials are underway in humans to establish the role of vitamin D in the prevention of cancers.
Vitamin D insufficiency may increase the risk for type I and type II diabetes mellitus. [34, 54] In NHANES III, lower vitamin D status was associated with higher fasting glucose and 2-hour glucose after an oral glucose tolerance test. [55] Furthermore, vitamin D supplementation in adults has been associated with improved insulin sensitivity in several small, case-control studies. [54]
Joergensen et al determined that vitamin D deficiency in type 1 diabetes may predict all causes of mortality but not development of microvascular complications. [56] The contribution of vitamin D deficiency to mortality must be mediated by nonvascular mechanisms.
A study by Li et al indicated that vitamin D deficiency (serum 25-hydroxyvitamin D < 12 ng/mL) is related to an increased stroke risk in adults, with an association also found between higher vitamin D levels and a reduced stroke risk. The study, on adults aged 20 years or older, found that evidence for the relationship between high serum 25-hydroxyvitamin D levels and decreased stroke risk was particularly strong among females below age 50 years. [57]
Low levels of vitamin D have also been linked to increased cardiovascular disease (CVD) biomarkers in older adults. In an observational study of 957 hypertensive older adults, vitamin D deficiency (< 25 nmol/L) was associated with higher levels of biomarkers linked with CVD and conditions such as multiple sclerosis and rheumatoid arthritis. [58, 59, 60] Individuals deficient in vitamin D had significantly higher levels of the inflammatory biomarkers interleukin-6 (IL-6) and C-reactive protein (CRP), and higher IL-6:IL-10 and CRP:IL-10 ratios compared with subjects who had serum vitamin D levels > 75 nmol/L. [58, 59]
A meta-analysis evaluated the effect of vitamin D supplementation (using a mean supplementation dosage of about 500 IU daily) on all-cause mortality in 18 randomized controlled trials and found a 7% relative risk reduction for death. [61] Severe vitamin D deficiency (25(OH)D < 10 ng/mL) has been associated with increased in-hospital mortality in patients admitted for acute coronary syndrome. [62]
Low vitamin D in patients with coronavirus disease 2019 (COVID-19) reflects a heightened inflammatory state and possibly could be used as a surrogate marker for high risk of severe disease. [63]
A retrospective, observational study by De Smet et al indicated that patients with COVID-19 who have vitamin D deficiency at hospital admission have an almost four-fold greater chance of mortality from COVID-19. This increase occurred independently of age, ethnicity, the presence of chronic lung disease, or the degree of lung damage (as determined through chest computed tomography [CT] scan severity score). [64, 65]
A Cochrane Review of 50 randomized, controlled trials that included more than 94,000 individuals, primarily elderly women, found that vitamin D3 supplementation decreased mortality. Other forms of vitamin D, including vitamin D2, calcitriol, and alpha-calcidiol, did not reduce mortality. [66]
A study by Manson et al to evaluate the efficacy of vitamin D supplementation and omega-3 fatty acids in lowering the risk of invasive cancer and cardiovascular disease found no such reduction associated with the administration of vitamin D. The report, which included 25,871 participants (males aged 50 years or older and females aged 55 years or older) and had a median follow-up period of 5.3 years, determined that compared with a placebo group, there was no decrease in the incidence of breast, prostate, or colorectal cancer, or in myocardial infarction, stroke, or cardiovascular-related death, among subjects who consumed 2000 IU per day in supplementary vitamin D. [67]
![]()
-
Hollis BW, Wagner CL. Normal serum vitamin D levels. N Engl J Med. 2005 Feb 3. 352(5):515-6; author reply 515-6. [Medline].
-
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2011 Jun 6. [Medline].
-
Weishaar T, Rajan S, Keller B. Probability of Vitamin D Deficiency by Body Weight and Race/Ethnicity. J Am Board Fam Med. 2016 Mar-Apr. 29 (2):226-32. [Medline]. [Full Text].
-
Haddad JG, Matsuoka LY, Hollis BW, Hu YZ, Wortsman J. Human plasma transport of vitamin D after its endogenous synthesis. J Clin Invest. 1993 Jun. 91(6):2552-5. [Medline]. [Full Text].
-
Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008 Apr. 87(4):1080S-6S. [Medline].
-
Tangpricha V, Koutkia P, Rieke SM, et al. Fortification of orange juice with vitamin D: a novel approach for enhancing vitamin D nutritional health. Am J Clin Nutr. 2003 Jun. 77(6):1478-83. [Medline]. [Full Text].
-
Holick MF. Vitamin D deficiency: what a pain it is. Mayo Clin Proc. 2003 Dec. 78(12):1457-9. [Medline].
-
Heaney RP, Dowell MS, Hale CA, et al. Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr. 2003 Apr. 22(2):142-6. [Medline]. [Full Text].
-
Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab. 2004 Nov. 89(11):5387-91. [Medline]. [Full Text].
-
Trang HM, Cole DE, Rubin LA, et al. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am J Clin Nutr. 1998 Oct. 68(4):854-8. [Medline]. [Full Text].
-
Holick MF, Biancuzzo RM, Chen TC, et al. Vitamin D2 is as effective as vitamin D3 in maintaining circulating concentrations of 25-hydroxyvitamin D. J Clin Endocrinol Metab. 2008 Mar. 93(3):677-81. [Medline].
-
Phillips D. Maternal Vitamin D Status Tied to Long-term Outcomes in Kids. Medscape. 2014 Dec 16. [Full Text].
-
Hart PH, Lucas RM, Walsh JP, Zosky GR, Whitehouse AJ, Zhu K, et al. Vitamin D in Fetal Development: Findings From a Birth Cohort Study. Pediatrics. 2014 Dec 15. [Medline].
-
Kamudoni P, Poole C, Davies SJ. An estimate of the economic burden of vitamin D deficiency in pregnant women in the United Kingdom. Gynecol Endocrinol. 2016 Mar 29. 1-6. [Medline].
-
Bouillon R, Marcocci C, Carmeliet G, et al. Skeletal and extra-skeletal actions of vitamin D: current evidence and outstanding questions. Endocr Rev. 2018 Oct 12. [Medline].
-
Liu BA, Gordon M, Labranche JM, et al. Seasonal prevalence of vitamin D deficiency in institutionalized older adults. J Am Geriatr Soc. 1997 May. 45(5):598-603. [Medline].
-
Tangpricha V, Luo M, Fernández-Estívariz C, et al. Growth hormone favorably affects bone turnover and bone mineral density in patients with short bowel syndrome undergoing intestinal rehabilitation. J Parenter Enteral Nutr. Nov-Dec 2006. 30:480-6. [Medline].
-
Koutkia P, Lu Z, Chen TC, Holick MF. Treatment of vitamin D deficiency due to Crohn's disease with tanning bed ultraviolet B radiation. Gastroenterology. 2001 Dec. 121(6):1485-8. [Medline].
-
Gartner LM, Greer FR. Prevention of rickets and vitamin D deficiency: new guidelines for vitamin D intake. Pediatrics. 2003 Apr. 111(4 Pt 1):908-10. [Medline]. [Full Text].
-
Elliott ME, Binkley NC, Carnes M, et al. Fracture risks for women in long-term care: high prevalence of calcaneal osteoporosis and hypovitaminosis D. Pharmacotherapy. 2003 Jun. 23(6):702-10. [Medline].
-
Thomas MK, Lloyd-Jones DM, Thadhani RI, et al. Hypovitaminosis D in medical inpatients. N Engl J Med. 1998 Mar 19. 338(12):777-83. [Medline]. [Full Text].
-
Tangpricha V, Pearce EN, Chen TC, et al. Vitamin D insufficiency among free-living healthy young adults. Am J Med. 2002 Jun 1. 112(8):659-62. [Medline].
-
Karalius VP, Zinn D, Wu J, et al. Prevalence of risk of deficiency and inadequacy of 25-hydroxyvitamin D in US children: NHANES 2003-2006. J Pediatr Endocrinol Metab. 2014 Mar 12. [Medline].
-
Reuters Staff. Vitamin D levels suboptimal for 1 in 10 US children. Reuters Health Information. April 10, 2014. [Full Text].
-
Shoben AB, Kestenbaum B, Levin G, Hoofnagle AN, Psaty BM, Siscovick DS, et al. Seasonal variation in 25-hydroxyvitamin d concentrations in the cardiovascular health study. Am J Epidemiol. 2011 Dec 15. 174(12):1363-72. [Medline].
-
van der Wielen RP, Löwik MR, van den Berg H, et al. Serum vitamin D concentrations among elderly people in Europe. Lancet. 1995 Jul 22. 346(8969):207-10. [Medline].
-
Gannagé-Yared MH, Chemali R, Yaacoub N, et al. Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J Bone Miner Res. 2000 Sep. 15(9):1856-62. [Medline].
-
Looker AC, Gunter EW. Hypovitaminosis D in medical inpatients. N Engl J Med. 1998 Jul 30. 339(5):344-5; author reply 345-6. [Medline].
-
Fuleihan GE, Deeb M. Hypovitaminosis D in a sunny country. N Engl J Med. 1999 Jun 10. 340(23):1840-1. [Medline].
-
Mishal AA. Effects of different dress styles on vitamin D levels in healthy young Jordanian women. Osteoporos Int. 2001. 12(11):931-5. [Medline].
-
Clemens TL, Adams JS, Henderson SL, et al. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet. 1982 Jan 9. 1(8263):74-6. [Medline].
-
Harris SS, Soteriades E, Coolidge JA, et al. Vitamin D insufficiency and hyperparathyroidism in a low income, multiracial, elderly population. J Clin Endocrinol Metab. 2000 Nov. 85(11):4125-30. [Medline]. [Full Text].
-
Nesby-O'Dell S, Scanlon KS, Cogswell ME, et al. Hypovitaminosis D prevalence and determinants among African American and white women of reproductive age: third National Health and Nutrition Examination Survey, 1988-1994. Am J Clin Nutr. 2002 Jul. 76(1):187-92. [Medline]. [Full Text].
-
Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004 Mar. 79(3):362-71. [Medline]. [Full Text].
-
Chapuy MC, Arlot ME, Duboeuf F, et al. Vitamin D3 and calcium to prevent hip fractures in the elderly women. N Engl J Med. 1992 Dec 3. 327(23):1637-42. [Medline].
-
Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ. 2003 Mar 1. 326(7387):469. [Medline]. [Full Text].
-
Boonen S, Lips P, Bouillon R, et al. Need for additional calcium to reduce the risk of hip fracture with vitamin d supplementation: evidence from a comparative metaanalysis of randomized controlled trials. J Clin Endocrinol Metab. 2007 Apr. 92(4):1415-23. [Medline]. [Full Text].
-
Bischoff-Ferrari HA, Willett WC, Wong JB, et al. Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch Intern Med. 2009 Mar 23. 169(6):551-61. [Medline].
-
Heaney RP. Vitamin D depletion and effective calcium absorption. J Bone Miner Res. 2003 Jul. 18(7):1342; author reply 1343. [Medline].
-
Dawson-Hughes B, Harris SS, Krall EA, et al. Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med. 1997 Sep 4. 337(10):670-6. [Medline]. [Full Text].
-
Harwood RH, Sahota O, Gaynor K, et al. A randomised, controlled comparison of different calcium and vitamin D supplementation regimens in elderly women after hip fracture: The Nottingham Neck of Femur (NONOF) Study. Age Ageing. 2004 Jan. 33(1):45-51. [Medline]. [Full Text].
-
Bischoff-Ferrari HA, Dietrich T, Orav EJ, et al. Positive association between 25-hydroxy vitamin D levels and bone mineral density: a population-based study of younger and older adults. Am J Med. 2004 May 1. 116(9):634-9. [Medline].
-
Bischoff HA, Stahelin HB, Dick W, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res. 2003 Feb. 18(2):343-51. [Medline].
-
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. 2009 Oct 1. 339:b3692. [Medline]. [Full Text].
-
Muir SW, Montero-Odasso M. Effect of vitamin d supplementation on muscle strength, gait and balance in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2011 Dec. 59(12):2291-300. [Medline].
-
Lappe JM, Travers-Gustafson D, Davies KM, et al. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007 Jun. 85(6):1586-91. [Medline]. [Full Text].
-
Chen TC, Holick MF. Vitamin D and prostate cancer prevention and treatment. Trends Endocrinol Metab. 2003 Nov. 14(9):423-30. [Medline].
-
Garland CF, Comstock GW, Garland FC, et al. Serum 25-hydroxyvitamin D and colon cancer: eight-year prospective study. Lancet. 1989 Nov 18. 2(8673):1176-8. [Medline].
-
Garland CF, Garland FC, Gorham ED. Calcium and vitamin D. Their potential roles in colon and breast cancer prevention. Ann N Y Acad Sci. 1999. 889:107-19. [Medline].
-
Garland FC, Garland CF, Gorham ED, et al. Geographic variation in breast cancer mortality in the United States: a hypothesis involving exposure to solar radiation. Prev Med. 1990 Nov. 19(6):614-22. [Medline].
-
Chen TC, Wang L, Whitlatch LW, et al. Prostatic 25-hydroxyvitamin D-1alpha-hydroxylase and its implication in prostate cancer. J Cell Biochem. 2003 Feb 1. 88(2):315-22. [Medline].
-
Freedman DM, Rajaraman P, Fuhrman B, et al. Sunlight, hormone replacement status and colorectal cancer risk in post-menopausal women. Int J Cancer. 2009 Sep 30. [Medline]. [Full Text].
-
Tangpricha V, Flanagan JN, Whitlatch LW, et al. 25-hydroxyvitamin D-1alpha-hydroxylase in normal and malignant colon tissue. Lancet. 2001 May 26. 357(9269):1673-4. [Medline].
-
Mathieu C, Gysemans C, Giulietti A, et al. Vitamin D and diabetes. Diabetologia. 2005 Jul. 48(7):1247-57. [Medline].
-
Scragg R, Sowers M, Bell C. Serum 25-hydroxyvitamin D, ethnicity, and blood pressure in the Third National Health and Nutrition Examination Survey. Am J Hypertens. 2007 Jul. 20(7):713-9. [Medline].
-
Joergensen C, Hovind P, Schmedes A, Parving HH, Rossing P. Vitamin d levels, microvascular complications, and mortality in type 1 diabetes. Diabetes Care. 2011 May. 34(5):1081-5. [Medline].
-
Li J, Lai H, Yang L, Zhu H, Chen S, Lai S. Age and Gender Differences in the Association between Serum 25-Hydroxyvitamin D and Stroke in the General US Population: The National Health and Nutrition Examination Survey, 2001-2006. J Stroke Cerebrovasc Dis. 2017 Nov. 26 (11):2510-8. [Medline].
-
Busko, M. Lack of Vitamin D Linked to CVD Biomarkers, Inflammation. Medscape. 2014 Feb 27. [Full Text].
-
Laird E, McNulty H, Ward M et al. Vitamin D deficiency is associated with inflammation in older Irish adults. J Clin Endocrinol Metab. February 2014.
-
Lee YH, Bae SC. Vitamin D level in rheumatoid arthritis and its correlation with the disease activity: a meta-analysis. Clin Exp Rheumatol. 2016 Apr 6. [Medline].
-
Autier P, Gandini S. Vitamin D supplementation and total mortality: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Sep 10. 167(16):1730-7. [Medline].
-
Correia LC, Sodré F, Garcia G, Sabino M, Brito M, Kalil F, et al. Relation of Severe Deficiency of Vitamin D to Cardiovascular Mortality During Acute Coronary Syndromes. Am J Cardiol. 2012 Nov 20. [Medline].
-
Busko M. Low vitamin D in COVID-19 predicts ICU admission, poor survival. MDedge. 2020 Sep 18. [Full Text].
-
McCall B. Vitamin D Deficiency in COVID-19 Quadrupled Death Rate. Medscape Medical News. 2020 Dec 11. [Full Text].
-
De Smet D, De Smet K, Herroelen P, Gryspeerdt S, Martens GA. Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality. Am J Clin Pathol. 2020 Nov 25. [Medline]. [Full Text].
-
Bjelakovic G, Gluud LL, Nikolova D, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2011 Jul 6. CD007470. [Medline].
-
Manson JE, Cook NR, Lee IM, et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N Engl J Med. 2019 Jan 3. 380 (1):33-44. [Medline]. [Full Text].
-
Chapuy MC, Preziosi P, Maamer M, et al. Prevalence of vitamin D insufficiency in an adult normal population. Osteoporos Int. 1997. 7(5):439-43. [Medline].
-
Herrmann M, Farrell CL, Pusceddu I, Fabregat-Cabello N, Cavalier E. Assessment of vitamin D status - a changing landscape. Clin Chem Lab Med. 2016 Jun 30. [Medline]. [Full Text].
-
Nainggolan L. Safe upper limit of vitamin D identified for first time. Medscape Medical News. May 1, 2013. [Full Text].
-
Dror Y, Giveon SM, Hoshen M, Feldhamer I, Balicer RD, Feldman BS. Vitamin d levels for preventing acute coronary syndrome and mortality: evidence of a nonlinear association. J Clin Endocrinol Metab. 2013 May. 98(5):2160-7. [Medline].
-
Bogh MK, Gullstrand J, Svensson A, Ljunggren B, Dorkhan M. Narrowband UVB three times a week more effective in treating vitamin D deficiency than 1600 IU oral vitamin D(3) /day: a randomized clinical trial. Br J Dermatol. 2012 May 25. [Medline].
-
Lu Z, Chen TC, Zhang A, et al. An evaluation of the vitamin D3 content in fish: is the vitamin D content adequate to satisfy the dietary requirement for vitamin D?. J Steroid Biochem Mol Biol. 2007 Mar. 103(3-5):642-4. [Medline].
-
Holick MF, Shao Q, Liu WW, et al. The vitamin D content of fortified milk and infant formula. N Engl J Med. 1992 Apr 30. 326(18):1178-81. [Medline].
-
Fox S. Vitamin D Supplements Found to Vary Widely in Potency. Medscape. 2013 Feb 11. [Full Text].
-
Hollis BW. Short-term and long-term consequences and concerns regarding valid assessment of vitamin D deficiency: comparison of recent food supplementation and clinical guidance reports. Curr Opin Clin Nutr Metab Care. 2011 Nov. 14(6):598-604. [Medline].
-
Brooks M. Proof Lacking for Routine Vitamin D Screening: US Task Force. Medscape Medical News. Jun 24 2014. [Full Text].
-
Perna L, Schöttker B, Holleczek B, Brenner H. Serum 25-hydroxyvitamin D and incidence of fatal and nonfatal cardiovascular events: a prospective study with repeated measurements. J Clin Endocrinol Metab. 2013 Dec. 98(12):4908-15. [Medline].
-
Tucker M. Vitamin D Deficiency Linked to Fatal CVD. Medscape. 2013 Dec 23. [Full Text].
Asthma And Vitamin D Deficiency In Adults
Source: https://emedicine.medscape.com/article/128762-overview





0 Komentar